

If you have ever lived with persistent, widespread pain that doctors find difficult to clearly explain, you are certainly not alone. Millions of people across the United States, from busy cities such as Houston and Chicago to coastal centres like Los Angeles and New York, struggle with chronic pain conditions every day. Two conditions that are frequently misunderstood or mistaken for one another are fibromyalgia and nerve pain, also known as neuropathic pain. Although they may appear similar because both can cause ongoing discomfort, fatigue, and sensitivity, they are actually quite different in terms of their underlying causes, how they are diagnosed, and the treatments doctors recommend.
Understanding these differences is important when exploring treatment options, including various pills for fibromyalgia pain and medications designed to calm irritated nerves. For example, the pregabalin tablet (commonly known as Lyrica) is a prescription anticonvulsant and gabapentinoid medicine primarily used to treat neuropathic pain, epilepsy, and certain anxiety disorders. Medicines like this target nerve signalling in the brain and spinal cord, helping reduce abnormal pain messages. In this guide, we will explain what fibromyalgia really is, how it differs from nerve pain, and which treatments may help people manage these challenging conditions more effectively.
What Is Fibromyalgia?
Fibromyalgia is a chronic disorder characterized by widespread musculoskeletal pain, extreme fatigue, sleep disturbances, and cognitive issues often called ‘fibro fog.’ Unlike many other pain conditions, fibromyalgia does not cause visible inflammation or tissue damage. Instead, it’s believed to involve the way the brain and spinal cord process pain signals — essentially, the nervous system becomes hypersensitive and amplifies ordinary sensations into painful ones.
According to the American College of Rheumatology, fibromyalgia affects an estimated 4 million adults in the United States. It’s commonly diagnosed in people between 30 and 60 years old, and it is far more prevalent in women than in men. In cities like Atlanta, Philadelphia, and Phoenix, it is one of the leading causes of chronic pain clinic visits every year.
Symptoms of Fibromyalgia in Women
Women make up approximately 80–90% of fibromyalgia diagnoses in the US. The symptoms of fibromyalgia in women can be distinct and more intense than in men. Common signs include:
- Widespread pain across multiple body regions, often described as a constant dull ache
- Extreme fatigue that doesn’t improve even after a full night’s sleep
- Morning stiffness lasting more than 15 minutes
- Headaches or migraines that recur frequently
- Painful menstrual cramps and heightened sensitivity during the menstrual cycle
- Irritable bowel syndrome (IBS) and digestive discomfort
- Memory lapses, poor concentration, and mental cloudiness (‘fibro fog’)
- Heightened sensitivity to light, noise, temperature, and touch
- Anxiety and depression, which often occur alongside the physical symptoms
Hormonal fluctuations appear to play a significant role in flare-up intensity for women, making symptoms especially difficult during perimenopause and menopause.
Is Fibromyalgia Hereditary?
One of the most common questions patients in cities like Seattle and Denver ask their doctors is: ‘Did I inherit this from my mother?’ Research suggests that fibromyalgia does have a genetic component. People who have a first-degree relative — such as a parent or sibling — with fibromyalgia are significantly more likely to develop the condition themselves.
However, fibromyalgia is not caused by a single gene. Scientists believe it results from a complex combination of genetic predisposition, environmental triggers, and psychological stress. Certain gene variations that affect serotonin, dopamine, and other neurotransmitter pathways may increase a person’s pain sensitivity, raising their risk of developing fibromyalgia when exposed to triggering events.
What Causes Fibromyalgia?
The exact cause of fibromyalgia is still not fully understood, but researchers and clinicians widely agree that it involves central sensitisation a state where the central nervous system becomes overactive and overly responsive to pain. Several triggers have been identified:
- Physical trauma or injury, such as a car accident or surgery
- Serious infections like Lyme disease or viral illness
- Post-traumatic stress disorder (PTSD) and prolonged emotional stress
- Sleep disorders that disrupt the body’s restorative processes
- Autoimmune conditions such as lupus or rheumatoid arthritis
- Hormonal imbalances, particularly in estrogen and cortisol
In many cases, no single triggering event can be identified. The condition may develop gradually over time, often leaving patients and doctors searching for answers for years before a diagnosis is made.
Fibromyalgia vs. Nerve Pain: The Key Differences
Neuropathic pain, or nerve pain, results from actual damage or dysfunction in the nervous system — either peripheral nerves (outside the brain and spinal cord) or the central nervous system itself. Conditions like diabetes, shingles, multiple sclerosis, and spinal injuries are common causes of nerve pain in the US.
Here’s how the two conditions differ in meaningful ways:
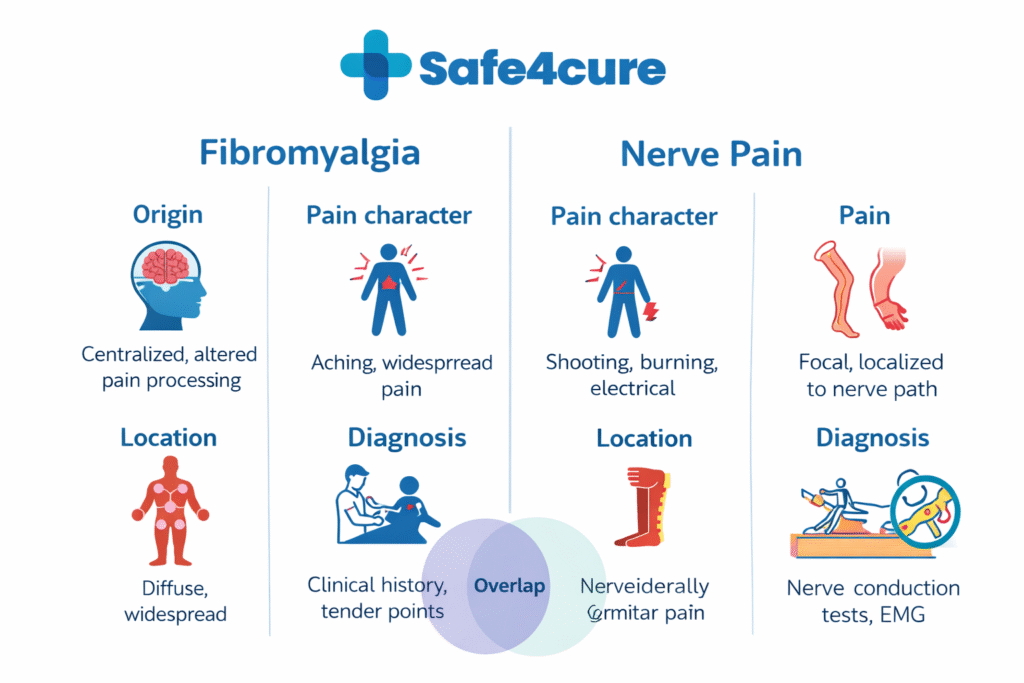
- Origin: Fibromyalgia arises from central nervous system hypersensitivity without structural nerve damage. Nerve pain involves actual injury or malfunction of specific nerves.
- Pain character: Fibromyalgia pain is typically widespread and aching. Nerve pain is often described as burning, stabbing, electric shock-like, or shooting.
- Location: Fibromyalgia affects multiple regions of the body. Nerve pain often follows a specific nerve pathway — for example, the sciatic nerve running down the leg.
- Diagnosis: Fibromyalgia is diagnosed clinically based on symptoms, history, and ruling out other conditions. Nerve pain can sometimes be confirmed with nerve conduction studies or imaging.
- Overlap: Both conditions can coexist. Someone with fibromyalgia may also experience nerve pain from an unrelated cause.
Pills for Fibromyalgia: What Are the Options?
Managing fibromyalgia often requires a multi-pronged approach, and medication plays an important role for many patients. The US Food and Drug Administration (FDA) has approved three medications specifically for fibromyalgia: duloxetine (Cymbalta), milnacipran (Savella), and pregabalin (Lyrica). Beyond these, doctors in cities like Miami, Dallas, and Boston often prescribe additional medications based on each patient’s symptom profile.
Common pill-based treatments include antidepressants that help regulate pain signals, muscle relaxants for stiffness, low-dose antiepileptics to calm overactive nerve pathways, and sleep aids to improve rest quality. Pain relievers like acetaminophen may also be recommended, while opioids are generally avoided as they have limited effectiveness for fibromyalgia and carry serious risks.
Pregabalin (Lyrica): A Key Medication for Nerve and Fibromyalgia
A pregabalin tablet — commonly known as Lyrica — is a prescription anticonvulsant and gabapentinoid medication primarily used to treat neuropathic pain, epilepsy, and anxiety. In the United States, pregabalin is legally classified as a Schedule V controlled substance due to risks of dependency, meaning it requires a valid prescription and careful medical supervision. In the UK, it is classified as a Class C controlled drug.
Pregabalin works by binding to calcium channels in the nervous system, which reduces the release of pain-transmitting neurotransmitters. This mechanism makes it effective at calming the overactive pain signals seen in both fibromyalgia and neuropathic conditions.
The pregabalin 300mg capsule is a commonly prescribed starting dose. Depending on the patient’s tolerance and response, doctors may gradually increase the dose over several weeks. Patients in cities like San Francisco and Chicago who are managing both fibromyalgia and neuropethic pain may find pregabalin to be particularly beneficial — but this medication must be only taken under a physician’s guidance due to the potential for side effects including dizziness, weight gain, and dependency.
Is Fibromyalgia a Disability?
This is a critically important question for many Americans living with severe fibromyalgia. The short answer is: yes, fibromyalgia can qualify as a disability under US law. The Social Security Administration (SSA) recognizes fibromyalgia as a legitimate medical condition that can prevent a person from maintaining full-time employment.
To qualify for Social Security Disability Insurance (SSDI) or Supplemental Security Income (SSI), a person with fibromyalgia must demonstrate that their condition significantly limits their ability to perform basic work activities. This requires detailed medical documentation, including records from rheumatologists, pain specialists, and primary care providers.
Thousands of fibromyalgia patients across the US — particularly in states like California, Florida, and Texas — have successfully obtained disability benefits after building a thorough medical record. If you’re considering this route, working with a disability attorney can significantly improve your chances of approval.
New Research and Emerging Treatments in the US
The landscape of fibromyalgia research is evolving rapidly. At institutions like the Mayo Clinic and Johns Hopkins, scientists are investigating the role of small fiber neuropathy in fibromyalgia — a subtle form of nerve damage that may help explain why some patients experience both fibromyalgia-like symptoms and true nerve pain. Skin biopsy testing for small fiber density is now available at several specialized centers across the country.
Another area of growing interest is the gut-brain connection. Researchers are finding that gut microbiome imbalances may contribute to central sensitization in fibromyalgia, opening the door to probiotic-based interventions as supportive therapy. Additionally, low-dose naltrexone (LDN) has gained traction in clinical circles as an off-label option that may reduce neuroinflammation and improve pain thresholds in fibromyalgia patients.
Transcranial magnetic stimulation (TMS), a non-invasive brain stimulation technique, is also being studied for its potential to reset pain processing patterns in fibromyalgia — with early results showing promise for fatigue and cognitive symptoms as well.
Living With Fibromyalgia: Practical Tips for Daily Management
Beyond medication, many patients find meaningful relief through lifestyle adjustments. Here are some strategies that specialists commonly recommend:
- Low-impact exercise: Swimming, walking, and yoga can significantly reduce pain and improve mood over time — even when starting very slowly.
- Sleep hygiene: Prioritizing consistent bedtimes and minimizing screen use before bed can dramatically affect symptom severity.
- Stress management: Cognitive behavioral therapy (CBT) has strong evidence behind it for fibromyalgia management, particularly in addressing the mental health dimensions.
- Pacing: Learning to balance activity and rest — rather than pushing through pain — helps prevent boom-and-bust cycles of overexertion followed by crash periods.
- Support networks: Joining fibromyalgia support groups, both in person in cities like Nashville and Portland, and online, can reduce isolation and provide practical coping strategies.
Frequently Asked Questions (FAQs)
Q1: Can fibromyalgia go away on its own?
Fibromyalgia is generally considered a long-term condition, but symptoms can fluctuate significantly over time. Some people experience long periods of remission where symptoms are minimal or manageable. With the right combination of treatment, lifestyle changes, and stress management, many patients achieve a much better quality of life than they had at diagnosis.
Q2: How is fibromyalgia diagnosed in the US?
There is no blood test or imaging scan that can confirm fibromyalgia. Diagnosis is based on clinical criteria, including widespread pain lasting more than three months, specific symptom severity scores, and ruling out other conditions through bloodwork and physical examination. A rheumatologist is typically the specialist who makes the diagnosis.
Q3: Is nerve pain the same as fibromyalgia?
No, they are different conditions. Nerve pain (neuropathic pain) results from actual damage or dysfunction in the nervous system, while fibromyalgia involves central sensitization without confirmed nerve damage. However, they can share overlapping symptoms and may coexist in the same person.
Q4: Is pregabalin safe for long-term use?
Pregabalin can be used long-term under a doctor’s supervision, but it requires regular monitoring due to its classification as a Schedule V controlled substance in the US. Long-term use may be associated with dependency, weight gain, and cognitive side effects. Never stop taking pregabalin abruptly without consulting your healthcare provider, as this can cause withdrawal symptoms.
Q5: Can men get fibromyalgia pain too?
Absolutely. While fibromyalgia is far more common in women, men do develop the condition. In fact, men with fibromyalgia are often underdiagnosed because the condition is frequently associated with women. Men tend to report pain differently, and symptoms may present with greater emphasis on fatigue and functional impairment rather than widespread pain.
